# Endocarditis
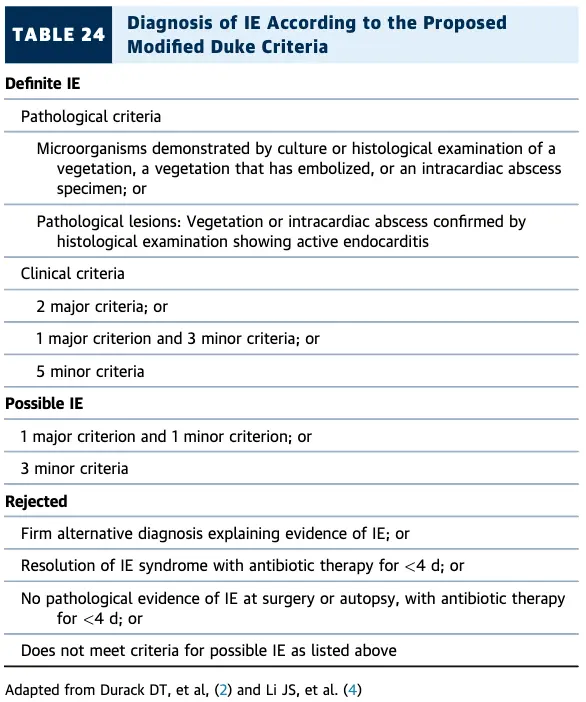
- Modified Duke Criteria: ***
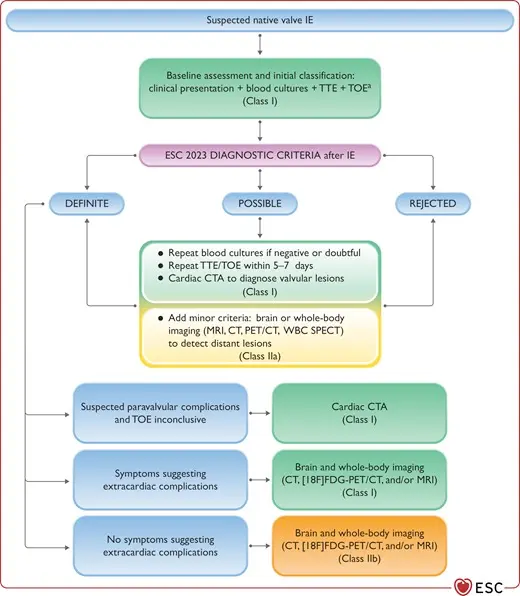
- If possible IE, plan for FGD-PET/CT
- BC x2
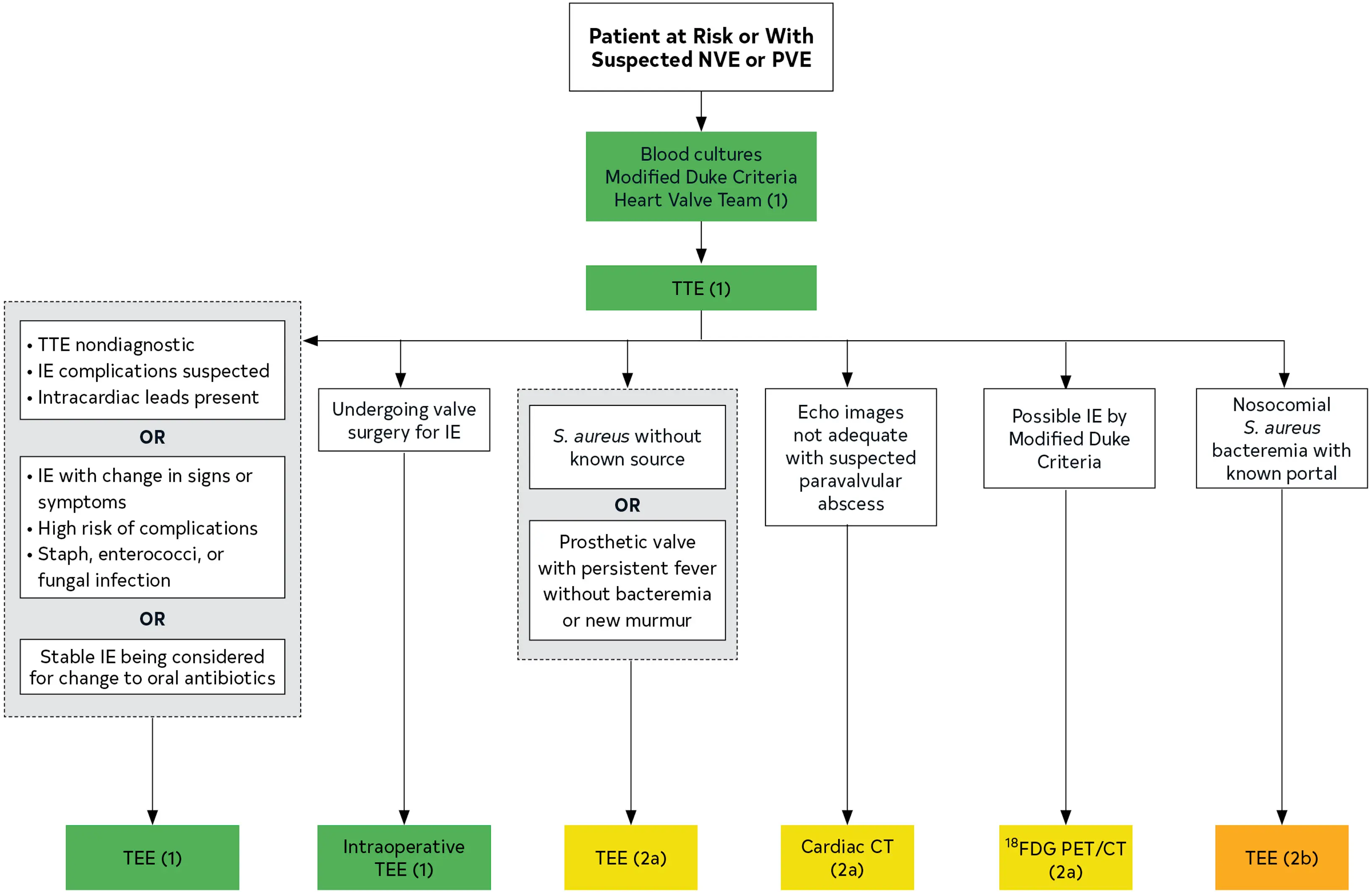
- TTE ordered to assess for vegetations, characterize the hemodynamic severity of valvular lesions, assess ventricular function and pulmonary pressures, and detect complications
- If TTE nondiagnostic, plan to proceed with TEE
- If paravalvular infection suspected, will order CT- Valves affected:
- MV > AV > TV > PV
- Microorganisms most commonly involved:
- Staph aureus (31%)
- Strep viridans (17%)
- Post-op: Staph epi early (within 2 months of valve surgery)
- Risk factors for IE:
- Age
- IVDU
- HD/IV lines
- Cancer
- Immunosuppression
- Structural heart disease
- Prosthetic valve/devices
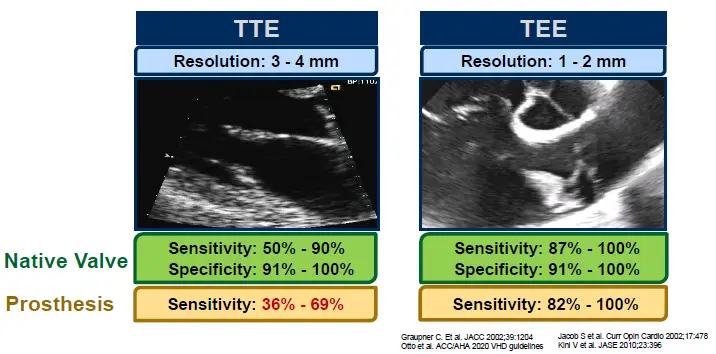
- TEE has better sensitivity for detecting bacterial endocarditis compared to TTE
- Native valve vs. Prosthetic valve? - Timing of infection after valve intervention?
- Fatal if untreated
- in-hospital mortality rate is 15% to 20%, with a 1-year mortality rate approaching 40% 1
Diagnosis
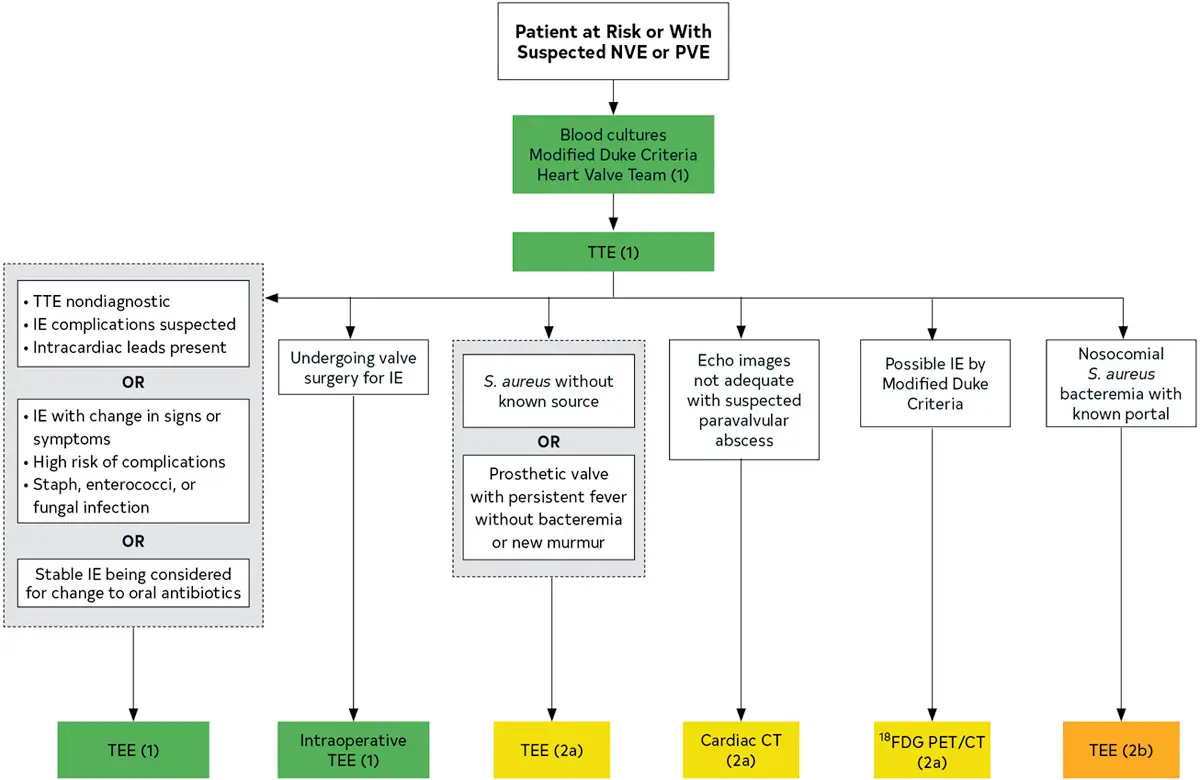 Figure source: 1
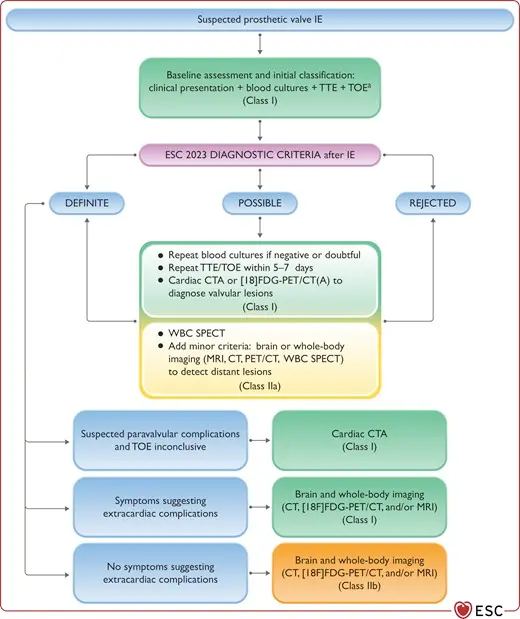
Figure source: 1
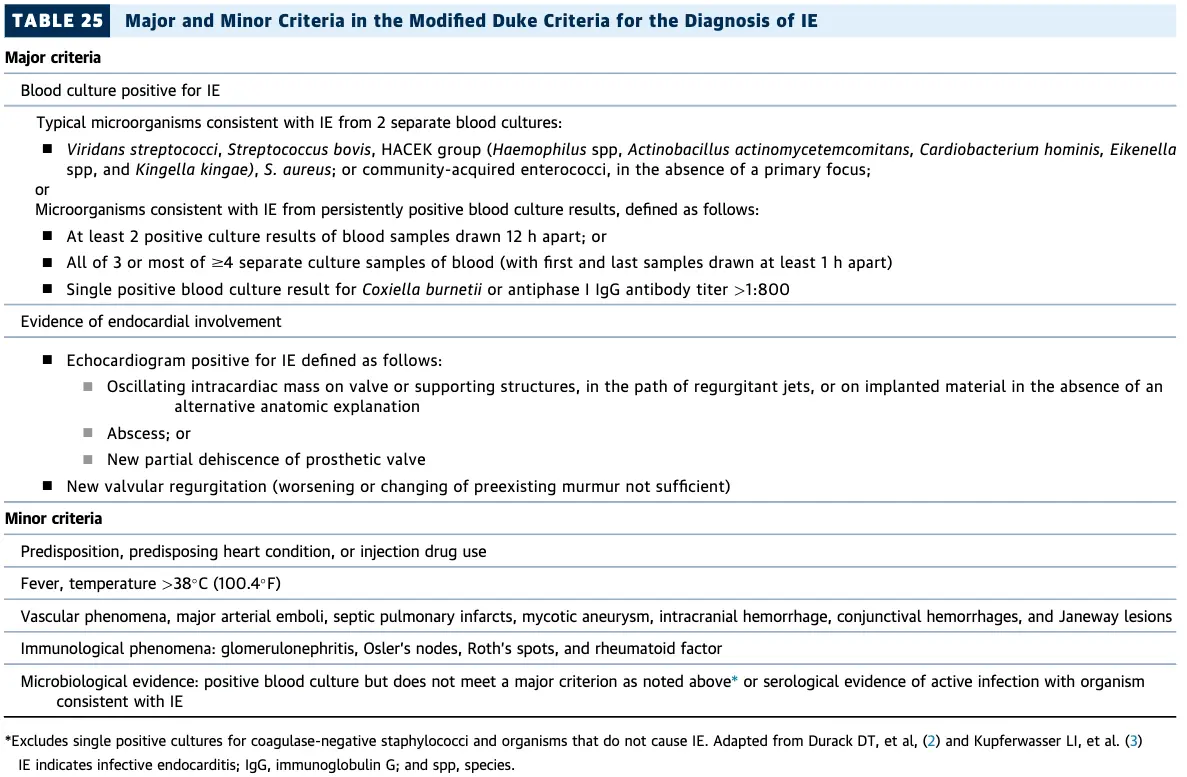
Modified Duke Criteria
Prosthetic Valve Endocarditis
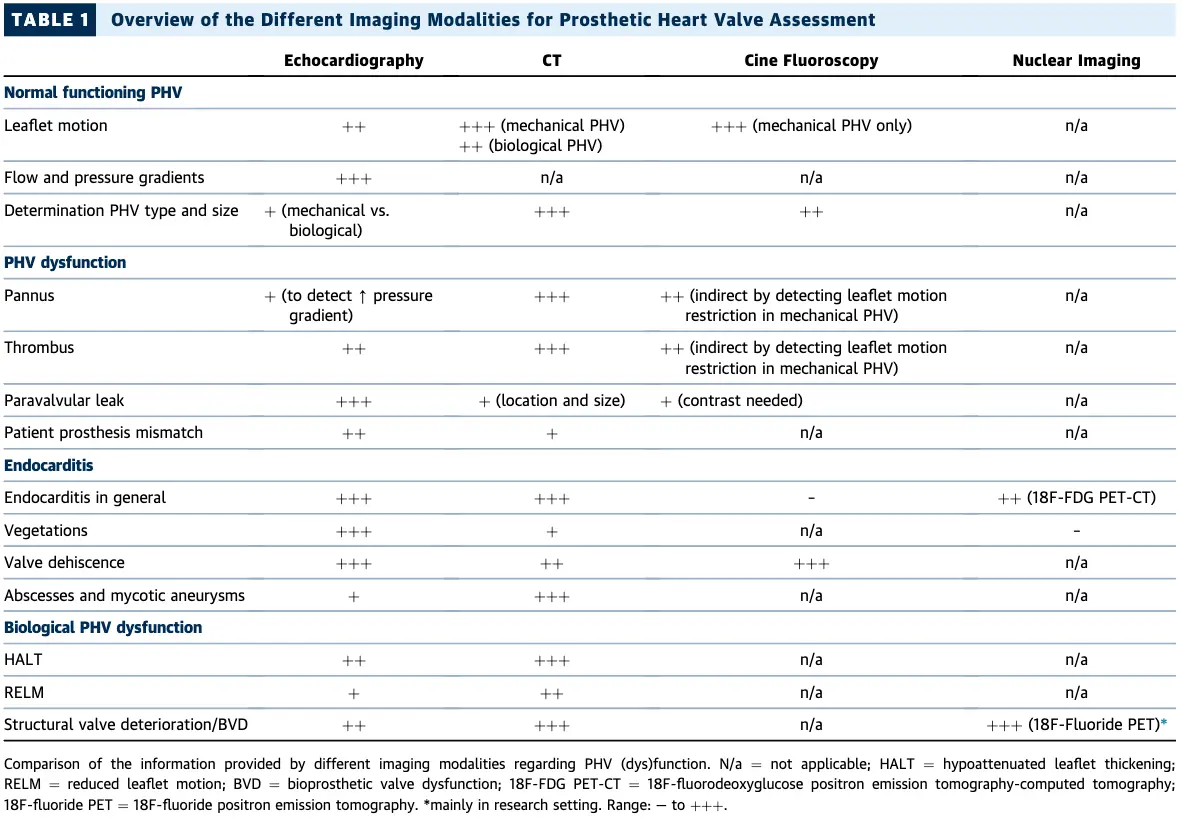 Table source: 2
Table source: 2
Opening and closing angles for different prosthetic valves:
 Table source: 2
Table source: 2
Echo
Prosthetic valve endocarditis (PVE) may have NO vegetation
⚠️ 30-40% cases of prosthetic valve endocarditis (PVE) have NO vegetation attached to the prosthesis, only peri-annular infection. ∴, you may want to consider TEE or other imaging modalities for PVE.
- Echo reports for IE should comment on the following:
- Diagnosis: confirm presence, location, size, number & morphology of the vegetation(s)
- Structural complications
- Local severity of valve destruction
- Impact on surrounding structures abscess, fistula, aneurysm, dehiscence
- Systemic embolization
- Hemodynamic impact
- Acute regurgitation, CHF, shunt, tamponade, valve obstruction, hemolysis
- TTE vs TEE
- TTE can pick up a vegetation as big as 3-4 mm, whereas TEE can pick up a veg as small as 1-2 mm
- Class I indications for TEE?
- Suspected IE +
- non-diagnostic TTE, suspect IE complications, intracardiac leads present OR
- IE with change in Si/Sx, high risk of complications, Infection with Staph/Strep/Enterococci
- Stable IE and considering switch from IV → PO Abx
- Suspected IE +
- DDx for mobile endocardial echodensity:
- Lambl’s excrescence, fenestration
- Vegetation: infective/non-infective (healed)
- e.g. Libman-Sacks endocarditis
- Sclerosis/calcium artifact, MAC
- Ruptured/retracted chordae
- Myxomatous tissue
- Valvular strands, surgical remnants
- Papillary fibroelastoma, myxoma
- Thrombus (e.g. prosthetic thrombosis)
- Characteristics of vegetations (Major criteria of Duke’s for “Evidence of endocardial involvement”)
- Motion:
- oscillating intracardiac mass on valve, supporting structures, or prosthesis; independent motion
- Effects:
- new regurgitation (worsening or changing or pre-existing murmur is not sufficient)
- abscess
- new partial dehiscence of prosthetic valve
- Location:
- Upstream side of the valve in the path of the regurgitant jet or on prosthetic material
- No alternative anatomic explanation
- Texture:
- Gray scale, similar reflectance of myocardium
- Shape:
- Lobulated and amorphous
- Motion:
Cardiac CTA
Management
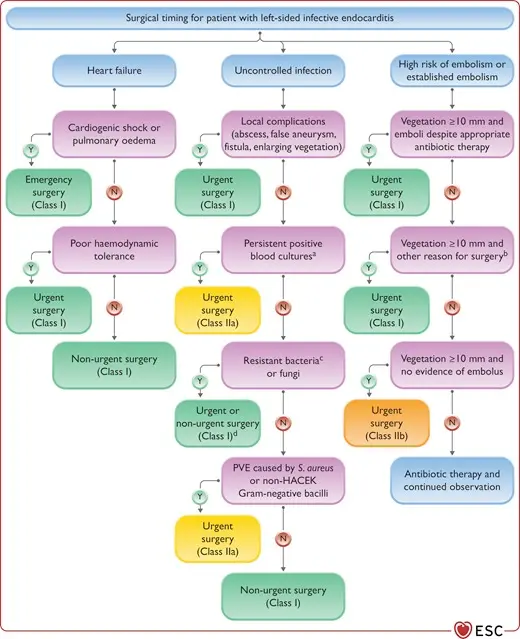
Complications
- Progression to involve the valve annulus → fistula between the LA and LV, which could result in significant regurgitation.
Footnotes
-
Otto, C. M., Nishimura, R. A., Bonow, R. O., Carabello, B. A., Erwin, J. P., Gentile, F., Jneid, H., Krieger, E. V., Mack, M., McLeod, C., O’Gara, P. T., Rigolin, V. H., Sundt, T. M., Thompson, A., & Toly, C. (2021). 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease. Journal of the American College of Cardiology, 77(4), e25–e197. https://doi.org/10.1016/j.jacc.2020.11.018 ↩ ↩2
-
Budde RPJ, Faure ME, Abbara S, Alkadhi H, Cremer PC, Feuchtner GM, Gonzales HM, Kiefer TL, Leipsic J, Nieman K, Revels J, Wang DD, Williamson E, Wyler von Ballmoos MC, Zwischenberger BA, Salgado R. Cardiac computed tomography for prosthetic heart valve assessment. An expert consensus document of the Society of Cardiovascular Computed Tomography (SCCT), the American College of Cardiology (ACC), the European Society of Cardiovascular Radiology (ESCR), the North American Society of Cardiovascular Imaging (NASCI), the Radiological Society of North America (RSNA), the Society for Cardiovascular Angiography & Interventions (SCAI) and Society of Thoracic Surgeons (STS). J Cardiovasc Comput Tomogr. 2025 Jul-Aug;19(4):366-386. doi: 10.1016/j.jcct.2025.04.007. Epub 2025 Jun 17. PMID: 40527640. ↩ ↩2