- Multisystem granulomatous disease
- Unknown etiology
- Results in arrhythmias, HF and SCD
- Second leading cause of sarcoidosis-related mortality
- #1 is pulmonary
- Increasing prevalence? Or are we just doing better with diagnosis?
- Diagnostic uncertainty is common
- Yield of EMB isn’t high b/c disease often patchy. EMB is the only way for us to be certain.
- Low NPV of EMB
- Risk stratification is challenging
- NOTE: isolated cardiac sarcoidosis is extremely rare, i.e. virtually non-existent. So always look out for extracardiac sarcoidosis.
Clinical presentation
- Unexplained AV block at <60 yo
- Unexplained ventricular arrhythmias
- Unexplained reduced LVEF
- Wall aneurysm/thinning in the absence of CAD
- ⚠️ We need to r/o CAD!
Diagnosis
- Diagnostic criteria
- HRS criteria
- TODO
- JCS criteria
- TODO
- WASOG criteria
- HRS criteria
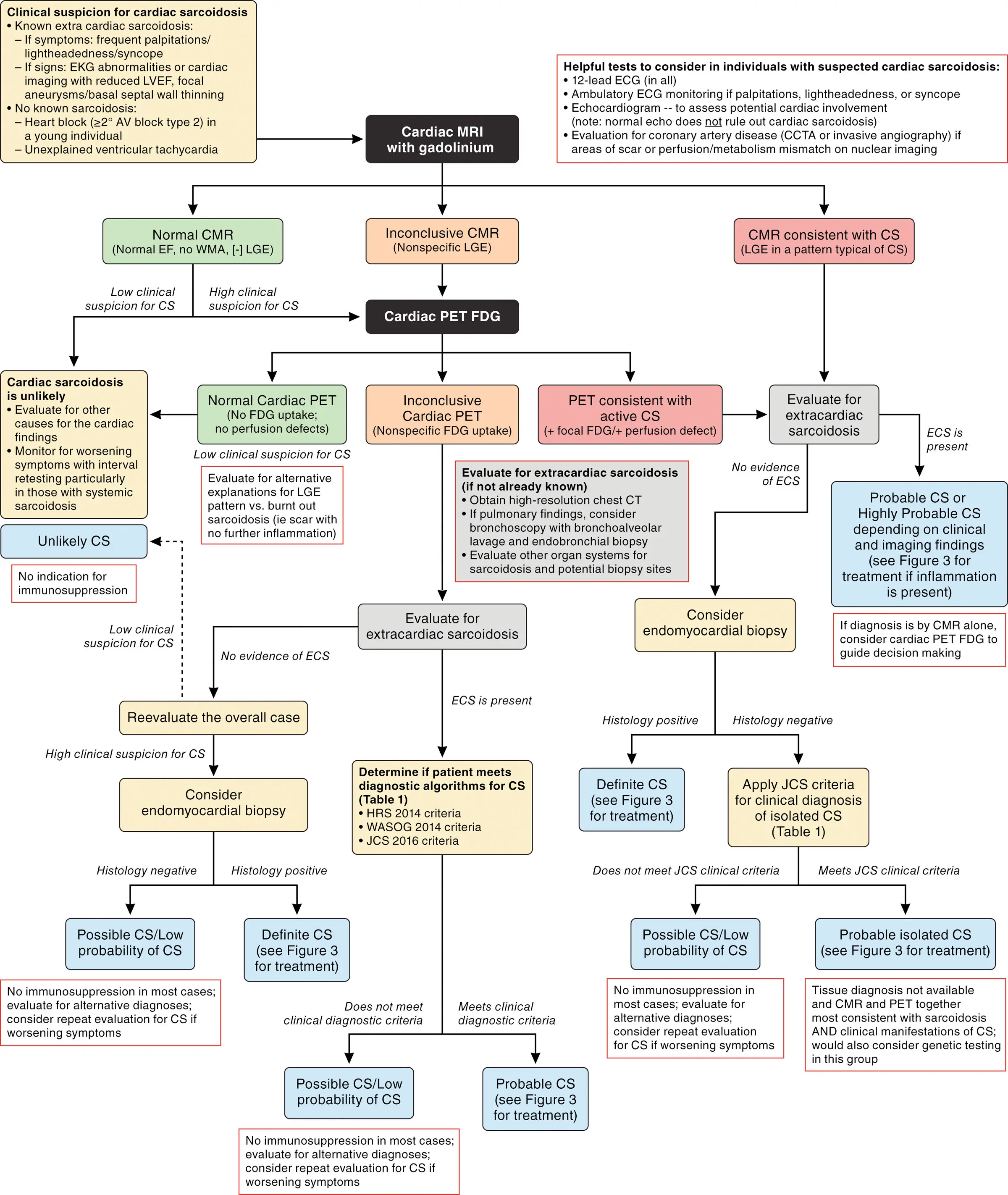
- The 2024 AHA Scientific Statement 1 is excellent for tying in multimodality imaging.
- MRI is great for ruling out cardiac sarcoidosis (MRI has high NPV). Get an MRI only if low clinical suspicion of cardiac sarcoidosis
- If you have high clinical suspicion, get an MRI + PET
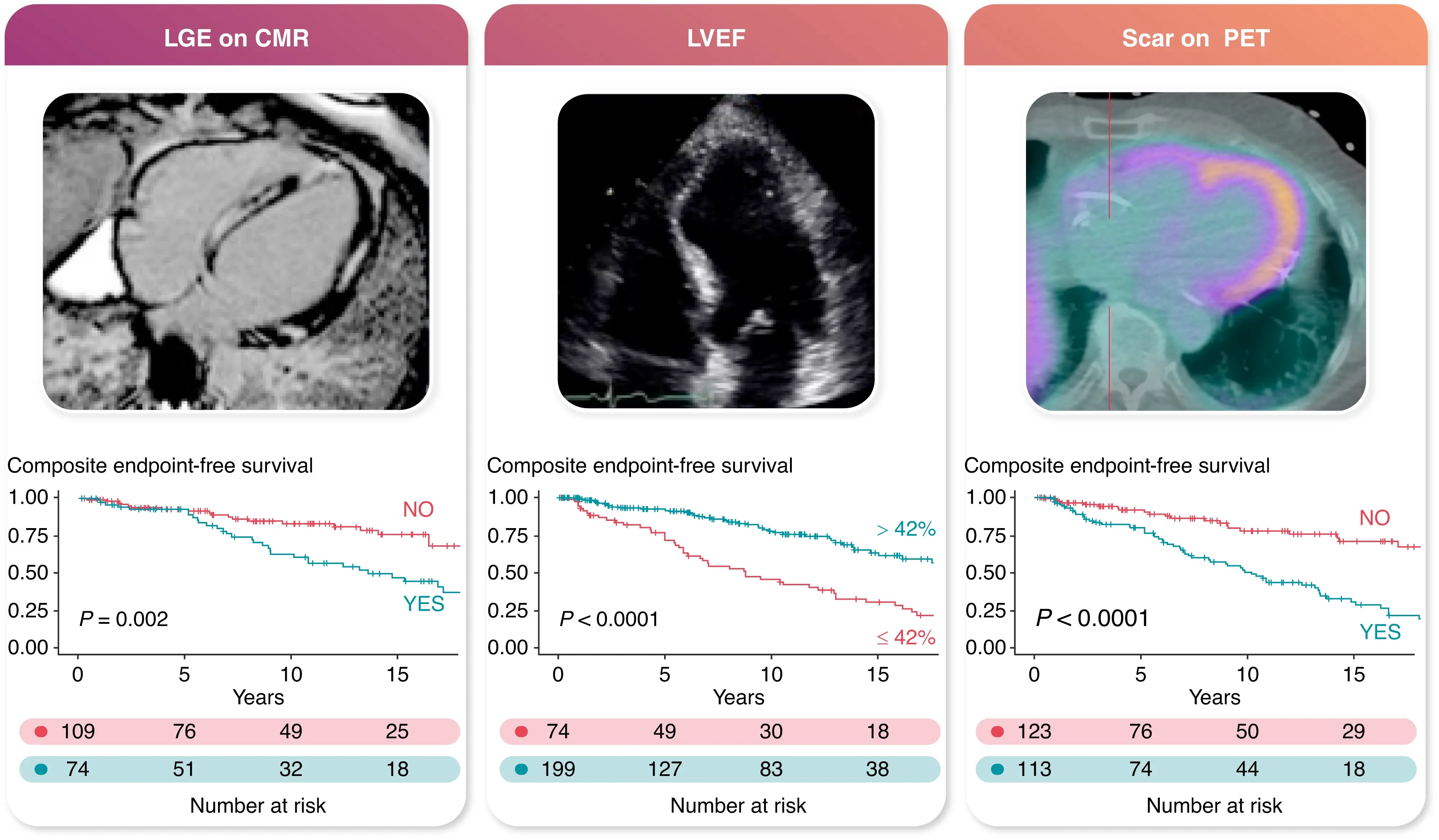 Figure source: 2
Figure source: 2
FDG-PET
- Assess disease activity and monitor therapy response
- Get every 3-6 months and guide therapy based on therapeutic response
- Whole body PET can identify extracardiac biopsy sites
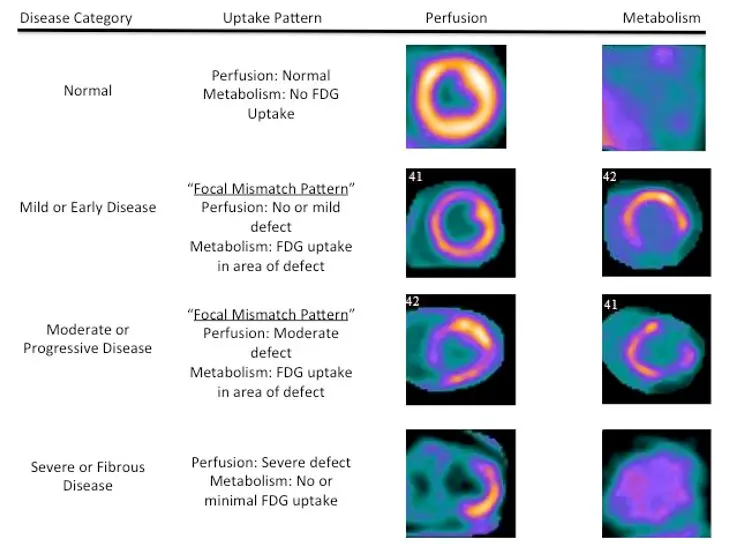
- Mismatch in perfusion and metabolism is highly specific (100%, 83% sensitive)
- Any FDG uptake pattern specificity can be as low as 33%
- Physiologic glucose metabolism may be heterogenous. For example, patients with LBBB or pacing can have non-specific lateral wall uptake.
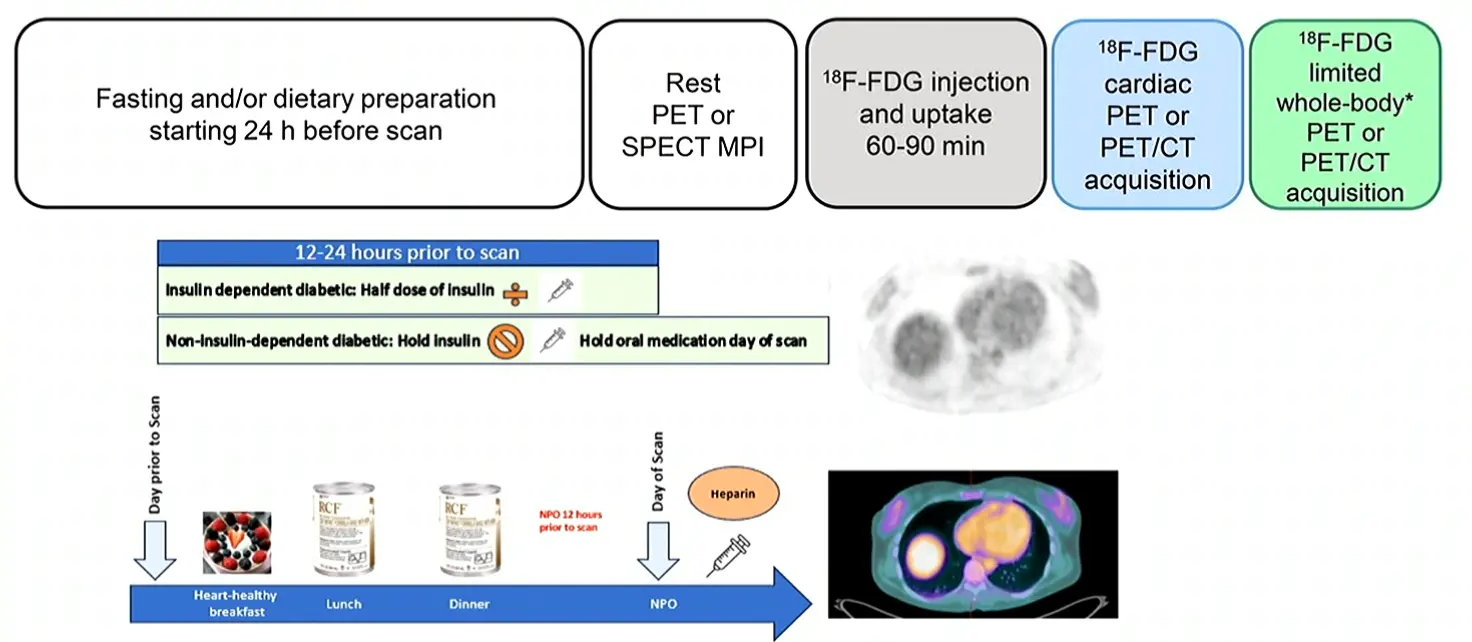
- Patient preparation is key 🔑
- It has to be endogenous ketosis, i.e. by fasting (KEE-TOSIS study)
- By limited they mean liver, spleen and entire heart.
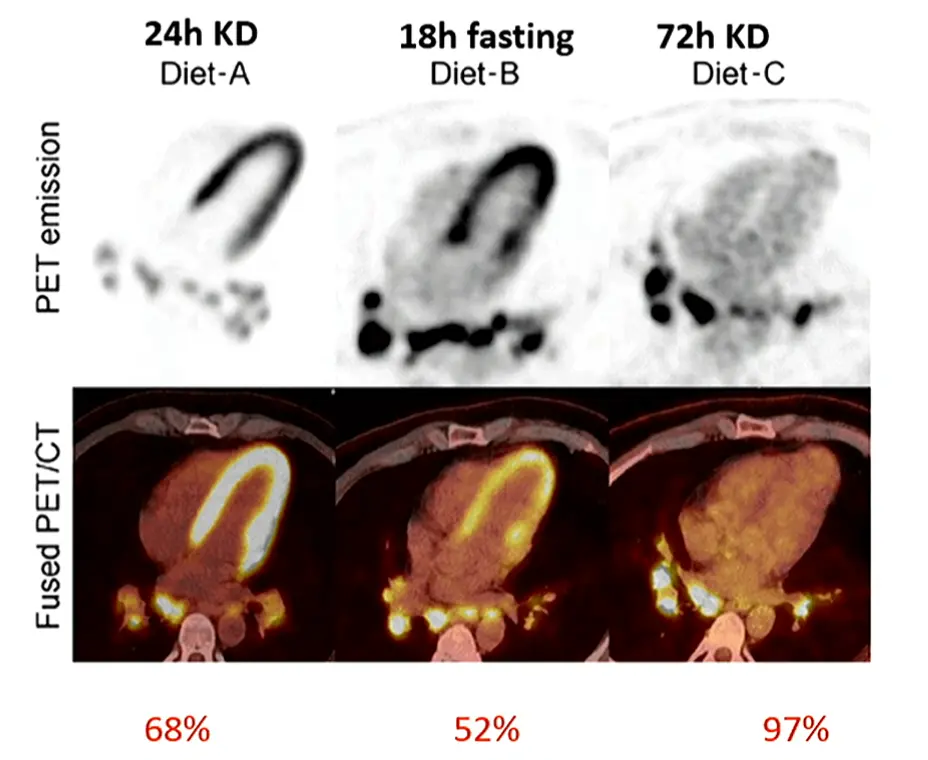
- Highlights that sometimes longer fasting yields better results (even if you have to go to 72 hours!)
- KEETO-CROSS study
- Injected ketones into the bloodstream didn’t work. We need endogenous ketosis.
- With high BHB levels, there was good correlation with the prep.
- They now consistently measure ketones before the prep.
- Must rule out ischemic heart disease
- b/c ischemic cells with take up FDG, which can be misleading. Ischemia induces translocation of GLUT4 to cell membrane
- Must r/o IHD b/c ischemic cells will uptake FDG - ischemic cells preferentially pickup glucose instead of free fatty acids
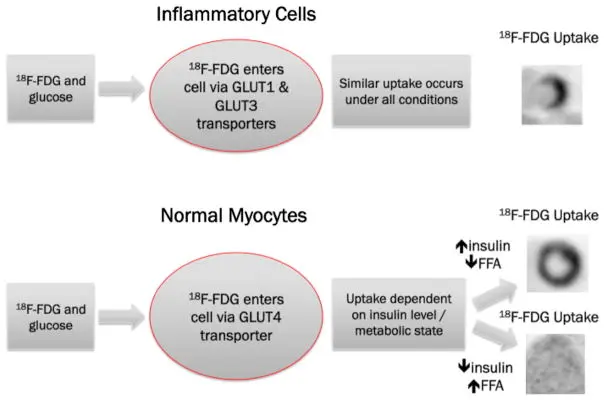 Figure source
Figure source
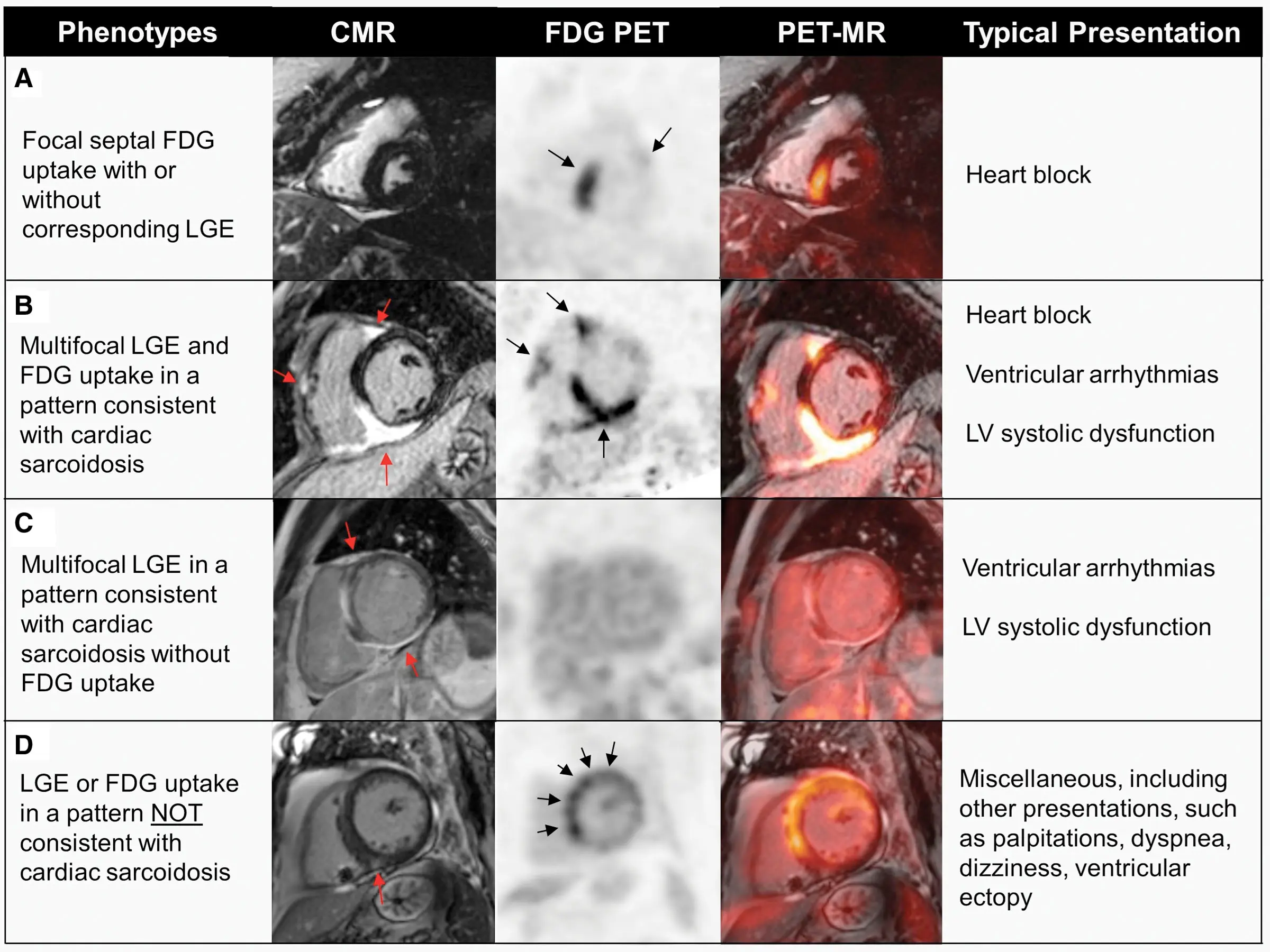 Figure source: 1
Figure source: 1
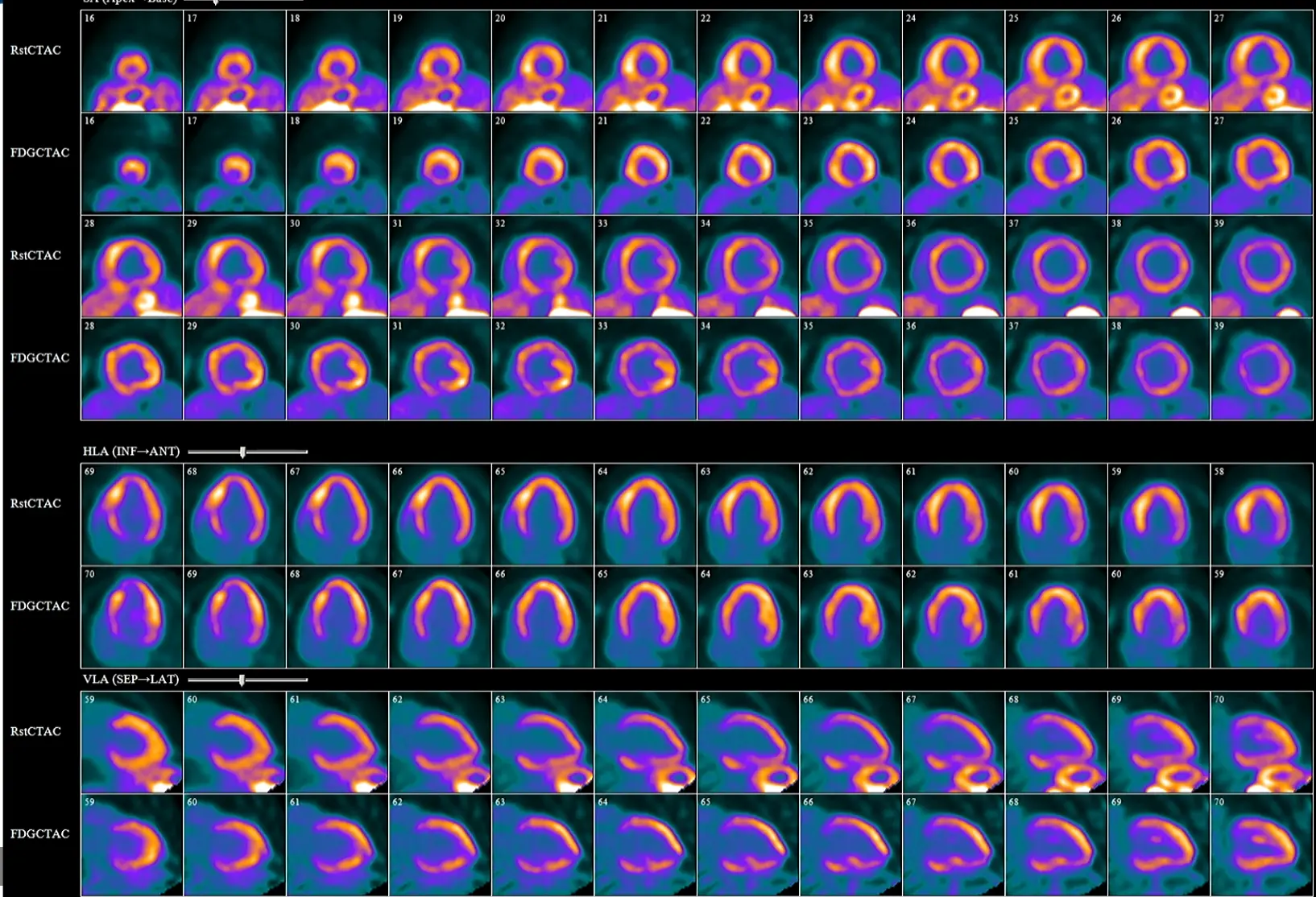
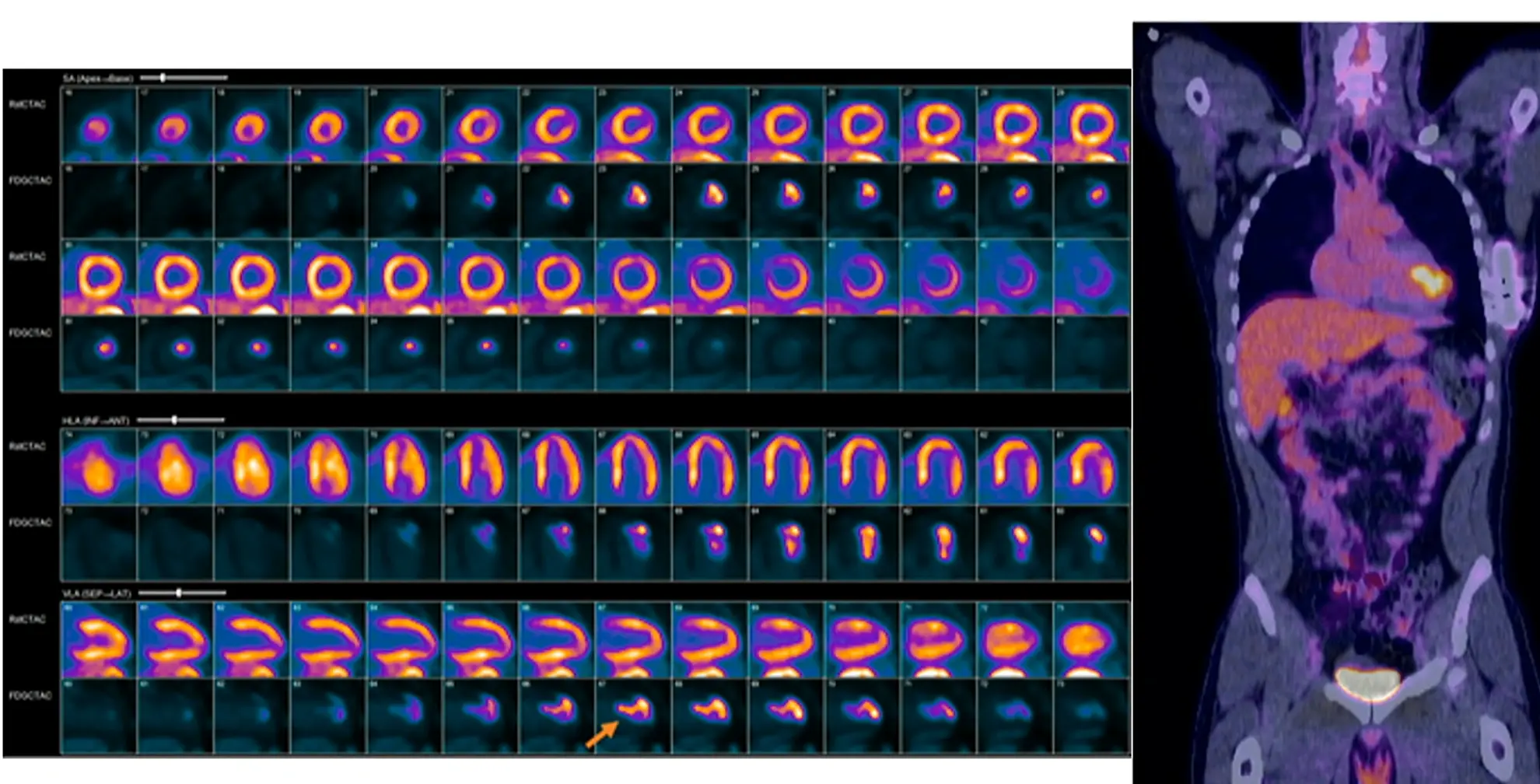
PET Example
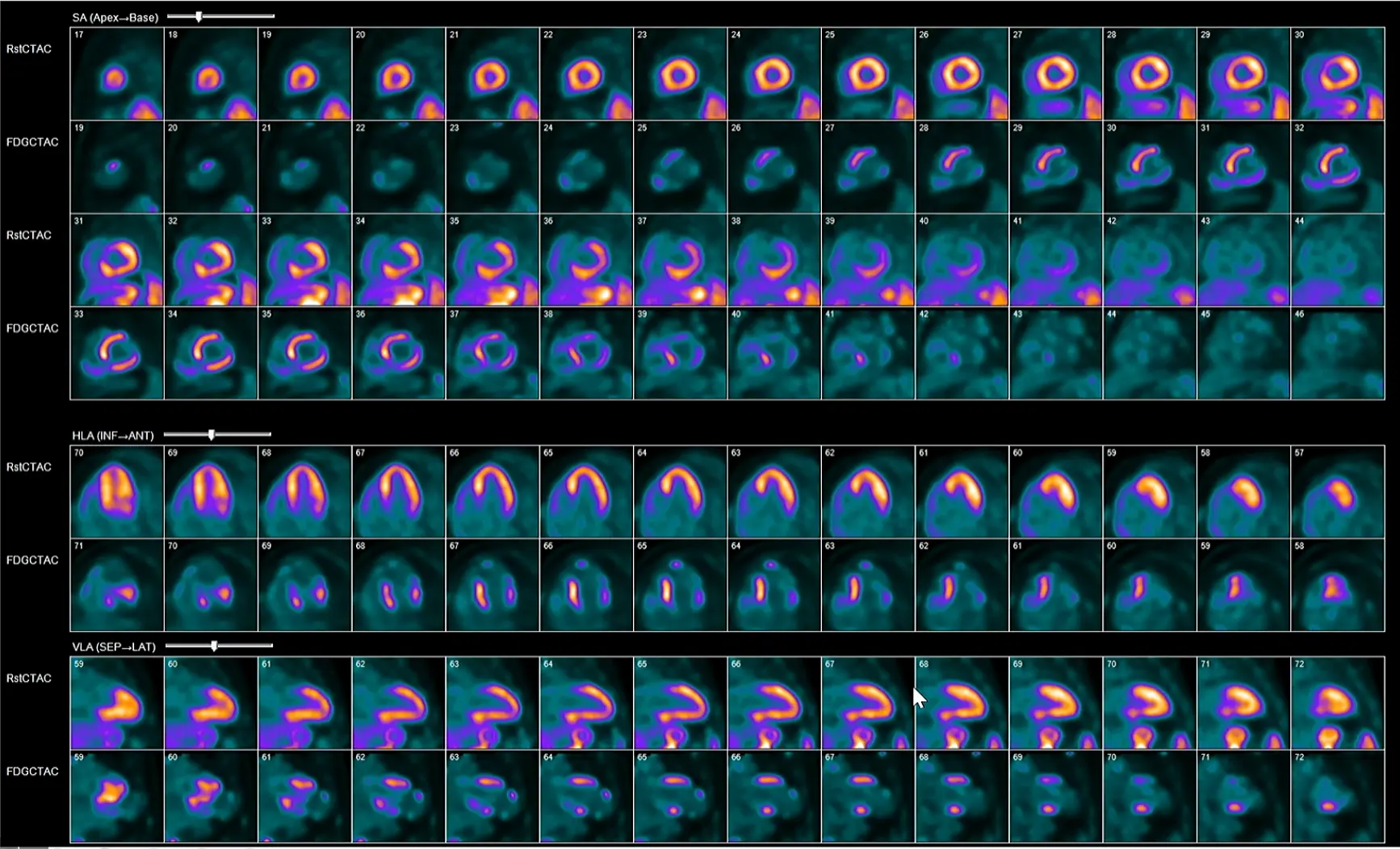
The example below shows a failure to suppress glucose uptake
Example of sarcoidosis that Hutt shared where cardiac sarcoidosis presented as an LV mass in a young patient. Initially thought hemangioma, but CT didn’t confirm this. They got transaortic biopsy expecting lymphoma, and the path showed sarcoidosis.
Whole Body PET
- Limited whole-body PET study using the same 18F-FDG injection should be performed in addition to the dedicated cardiac 18F-FDG study
- Should include the chest, liver, and spleen
- Can be interpreted even if poor dietary preparation or non-cardiac protocol
- Poor prep only affects cardiac glucose metabolism
- SUV of index nodes should be measured
- CT for AC can assess presence of LAD
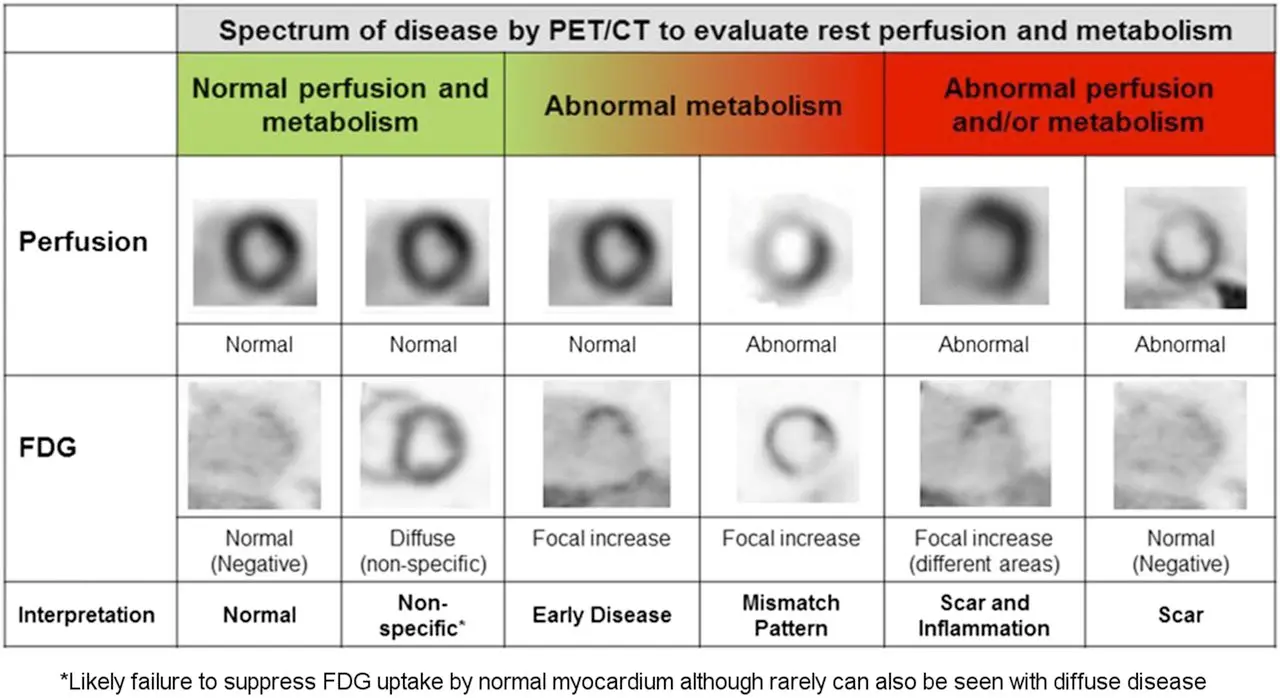
- Mismatch pattern is highly specific for sarcoidosis
- For diffuse non-specific (2nd column), more likely related to inappropriate suppression (probably poor prep)
MRI
- Step 1:
- 12-lead ECG
- Ambulatory ECG Monitoring
- Echocardiogram
- r/o CAD with a CCTA or cath
- CMR has a high NPV, so obtain CMR only in low clinical suspicion.
- Hutt gets it in patients with pulmonary sarcoid - 20% have cardiac sarcoid too and only 5% of them will have clinical manifestations of cardiac sarcoidosis.
- Obtain CMR and PET when high clinical suspicion
- Benefits:
- No preparation is needed
- May identify other causes of cardiomyopathy, e.g. dilated, genetic CM
- Ideally obtained at baseline, prior to PPM/ICD
- With pacemakers, artifact is minimal
- With ICD, hard to tell how much is artifact versus real LGE
- Wideband imaging decreases amount of artifact from the device
- If PPM is present, artifact tends to be minimal
- If ICD is present, artifact tends to be significant, and results are less accurate. Use wide band imaging and lift device as high as possible.
Interpretation with MRI:
- T1/2 mapping, T2-weighted edema imaging and LGE are most important sequences
- LGE carries the strongest prognostic value for SCD and arrhythmias
- 95% sensitivity, 85% specificity
- Typical pattern: multifocal multi-pattern LGE with septal and RV involvement. More specific but no pattern is 100% specific.
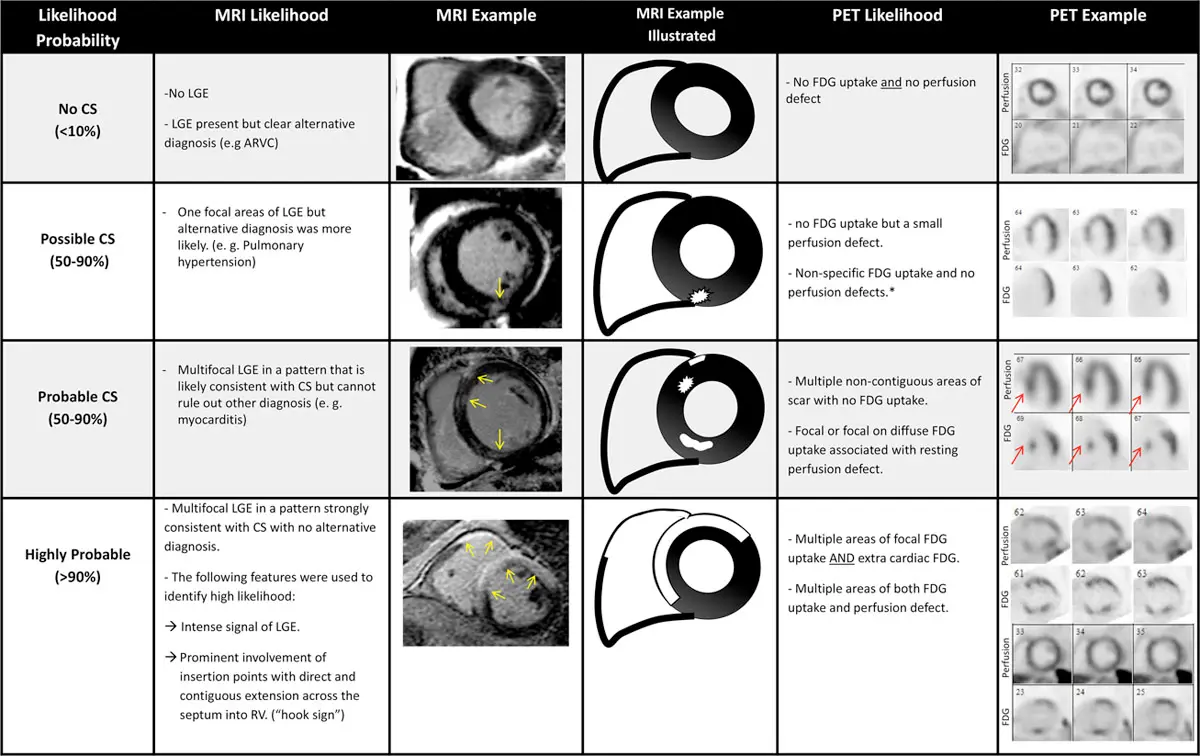
MRI Example
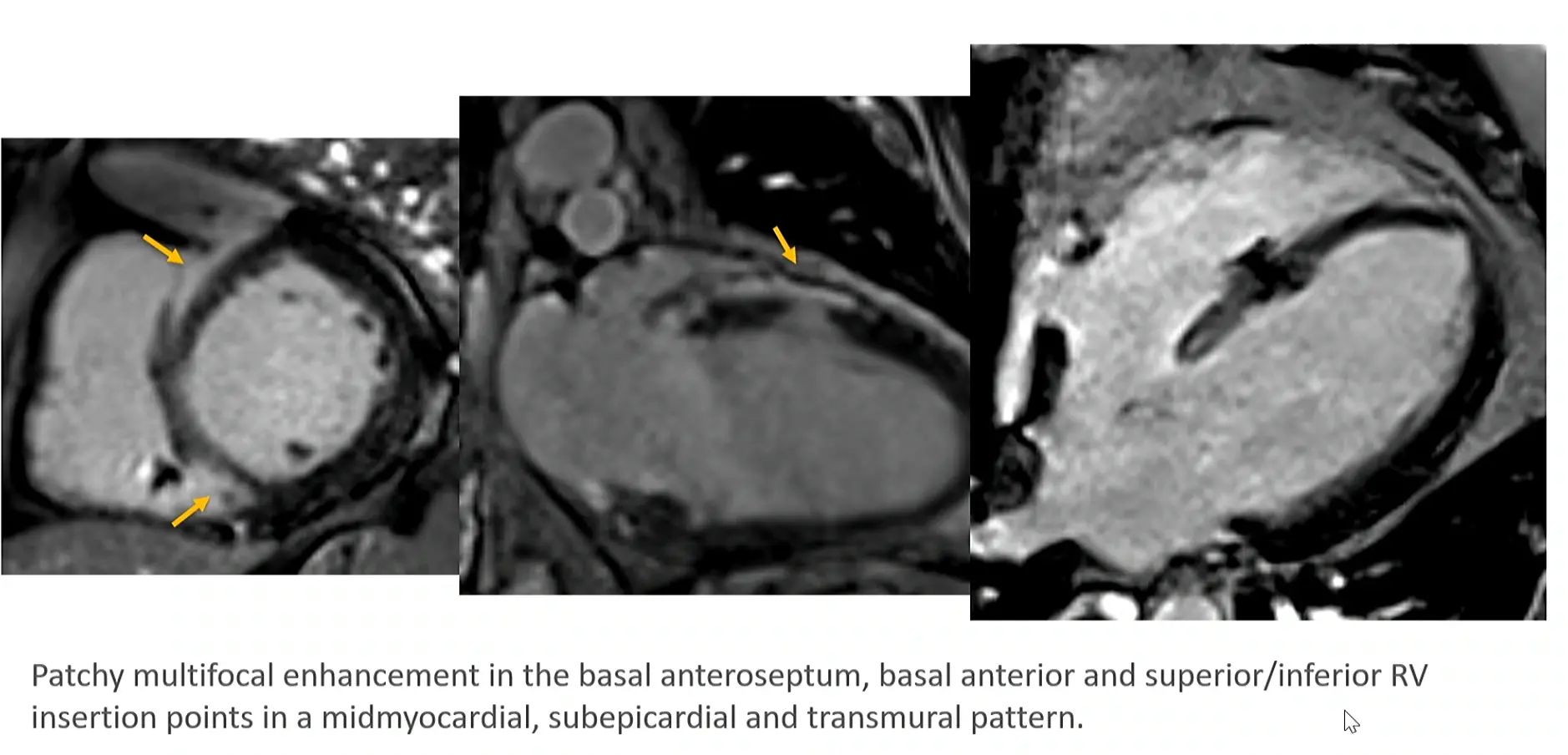
- Hutt described it as sometimes looking like someone taking a bite out of the myocardium.
Management
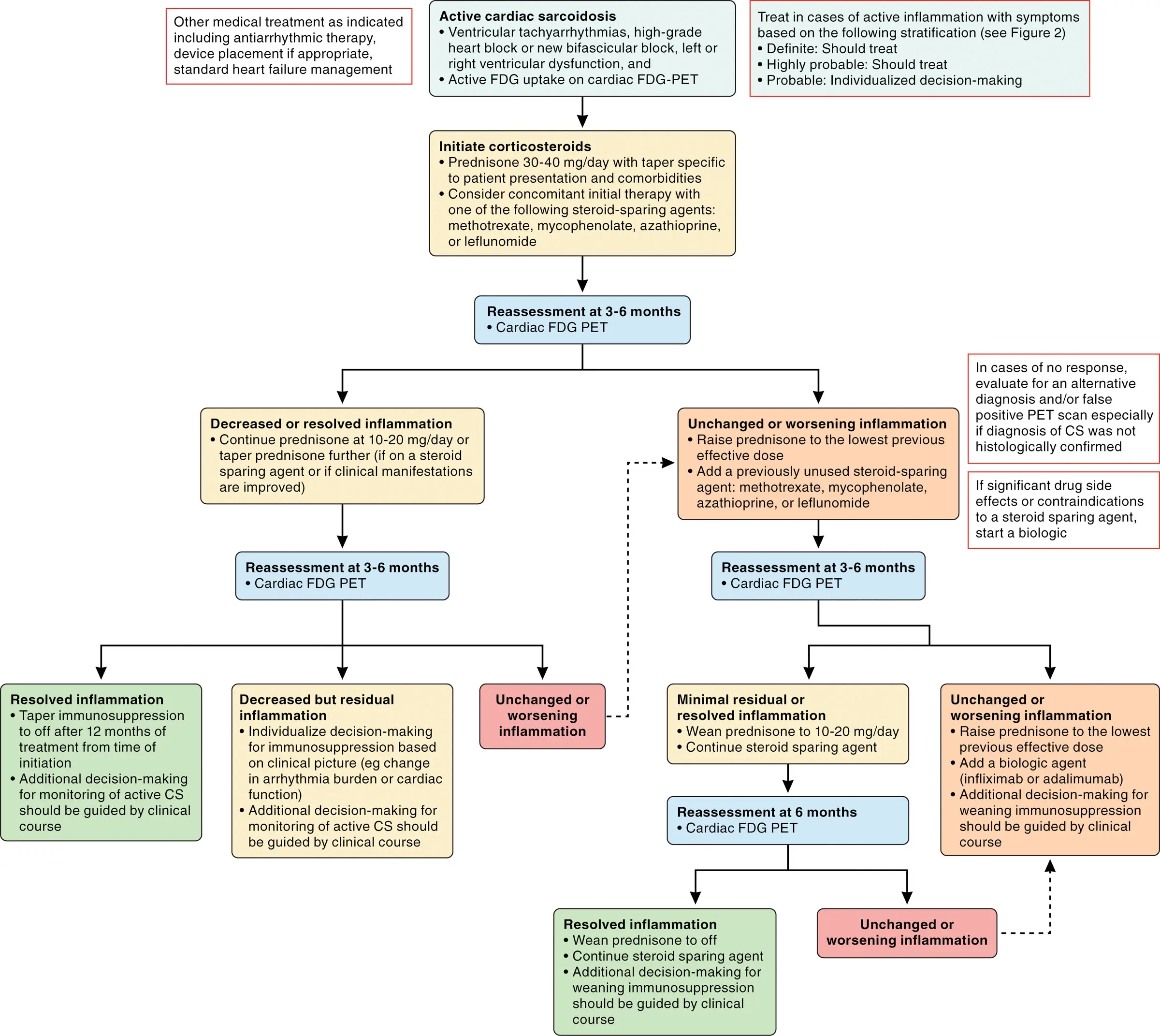 Figure source: 1
Figure source: 1
ICD
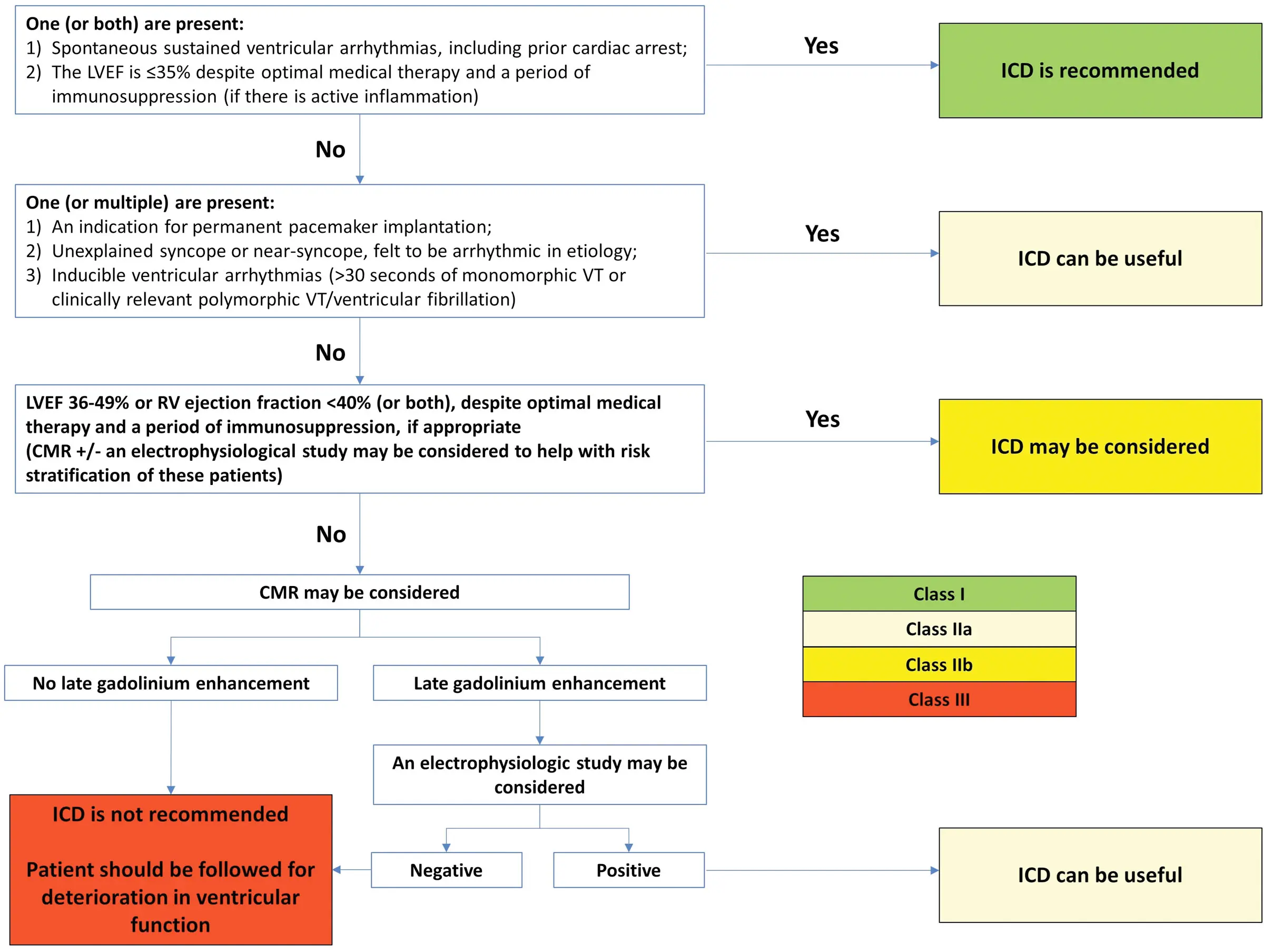 Figure source: 1
Figure source: 1
Footnotes
-
Cheng RK, Kittleson MM, Beavers CJ, Birnie DH, Blankstein R, Bravo PE, Gilotra NA, Judson MA, Patton KK, Rose-Bovino L; American Heart Association Heart Failure and Transplantation Committee of the Council on Clinical Cardiology, and Council on Cardiovascular and Stroke Nursing. Diagnosis and Management of Cardiac Sarcoidosis: A Scientific Statement From the American Heart Association. Circulation. 2024 May 21;149(21):e1197-e1216. doi: 10.1161/CIR.0000000000001240. Epub 2024 Apr 18. Erratum in: Circulation. 2024 Aug 20;150(8):e197. doi: 10.1161/CIR.0000000000001275. PMID: 38634276. ↩ ↩2 ↩3 ↩4
-
Hutt E, Brizneda MV, Goldar G, Aguilera J, Wang TKM, Taimeh Z, Culver D, Callahan T, Tang WHW, Cremer PC, Jaber WA, Ribeiro Neto ML, Jellis CL. Optimal left ventricular ejection fraction in risk stratification of patients with cardiac sarcoidosis. Europace. 2023 Aug 2;25(9):euad273. doi: 10.1093/europace/euad273. PMID: 37721485; PMCID: PMC10516712. ↩