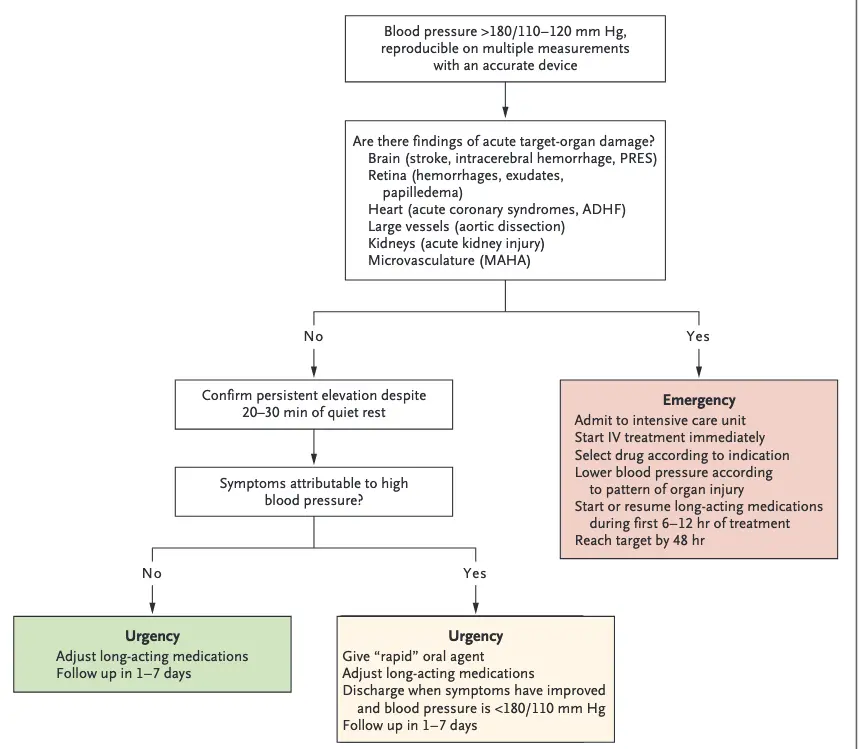
Hypertensive Urgency
- “For patients with symptoms that are presumed to relate to hypertension but are not indicative of target-organ damage (e.g., headache, atypical chest pain, or epistaxis), it is reasonable to choose an oral agent with a faster onset of action, such as clonidine (0.1 to 0.3 mg), labetalol (200 to 400 mg), captopril (25 to 50 mg), prazosin (5 to 10 mg), or nitroglycerin 2% topical ointment (1 to 2 in.). Nifedipine (given orally or sublingually) should be avoided owing to unpredictable blood-pressure reduction, possibly resulting in cardiovascular events. Medications can be administered every 30 minutes until the target blood pressure is achieved.”1
# Hypertensive Urgency
- Management:
- Nitropaste (NITROSTAT 2% ointment) 0.5 to 1 inch topical
- Captopril 25 to 50 mg
- Labetalol 200 to 400 mg
- Prazosin 5 to 10 mg
- Look out for relative bradycardia. If present, then maybe avoid an agent like labetalol
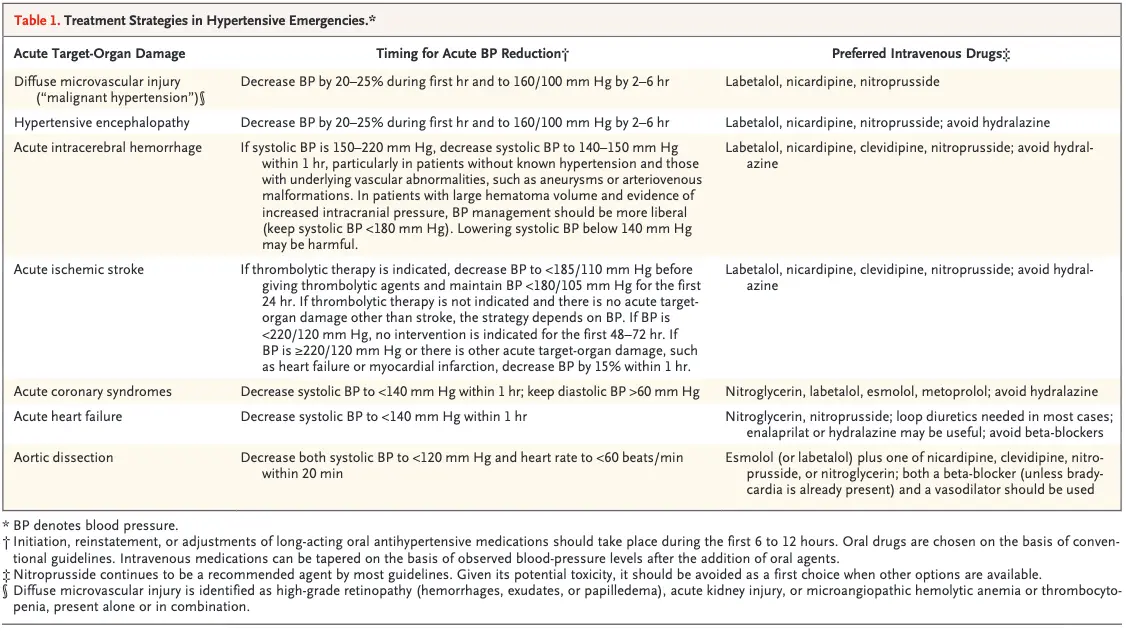
- BP should be decreased by no more than 20 to 25% during the first hour and then to 160/100-110 mmHg during the ensuing 2-6 hoursHypertensive Emergency
- Manage with IV anti-hypertensive medications
- The appropriate timing for starting or restarting oral drugs is uncertain; because the risk of hypotension is greatest in the first 6 hours of intravenous therapy, a reasonable approach is to start oral agents 6 to 12 hours after starting intravenous therapy.
- BP should be decreased by no more than 20 to 25% during the first hour and then to 160/100 to 110 mm Hg during the ensuing 2 to 6 hours.
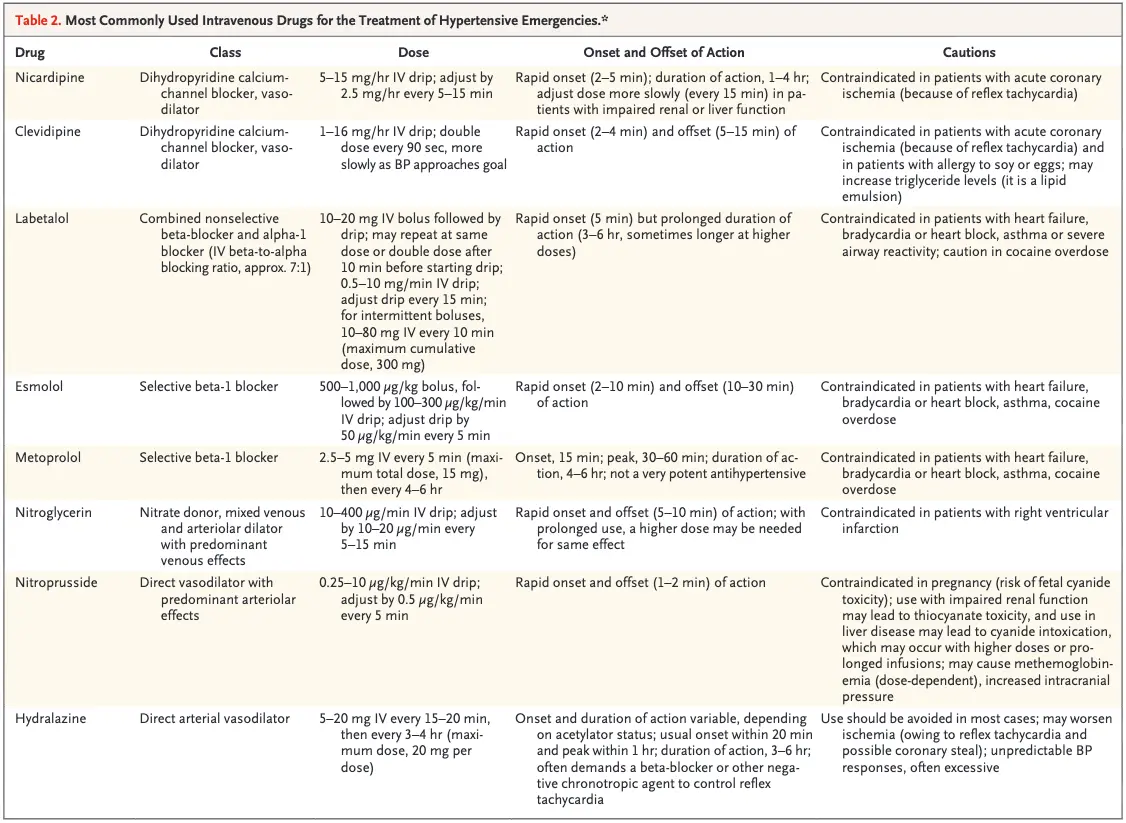
- In the United States, labetalol, nitroglycerin, nicardipine, hydralazine, and nitroprusside are the most commonly used agents.1
- Hydralazine has unpredictable effects, often leads to excessive blood-pressure lowering, and should generally be avoided as a first option