Electrical conduction typically begins in the sinus node located in the atrium and then travels to the atrioventricular node and down the bundle branches (conduction system) to allow coordinated filling and contraction of the ventricles.
Limb leads
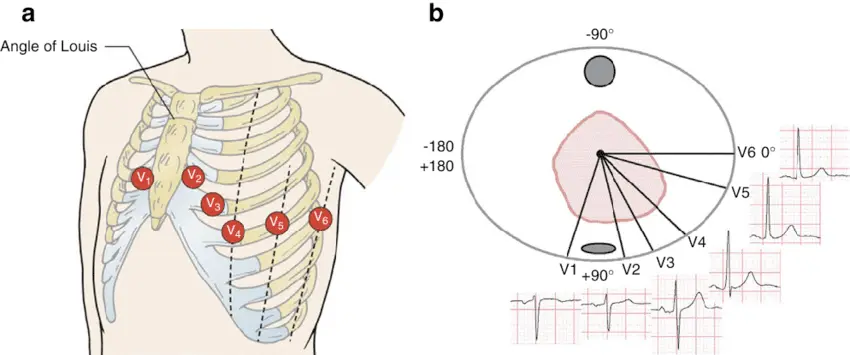
Precordial leads: V1-V6
Leads V1-V6 are unipolar leads that give you a perspective of cardiac activation from the anterior side of the heart.
Left leads: I and aVL
Right leads: V1 and aVR
📝 Under normal circumstances, the rhythm on the right and left leads will appear as mirror 🪞 images of one another.
∴ if you see a tiny Q-wave in the left-sided leads, you can expect to see an R-wave in the right-sided leads.
∴ if you see a big R-wave on the left-sided leads, you can expect to see an S-wave in the right-sided leads.
Normal activation
base → apex
endocardium → epicardium
In general, the left bundle is a thicker and a faster conducting structure (compared to the right bundle), so in a normal ventricle, you may expect to see tiny Q waves as the septum gets activated from left to right.
Most commonly seen normally in lateral leads (I, aVL, V5, V6)
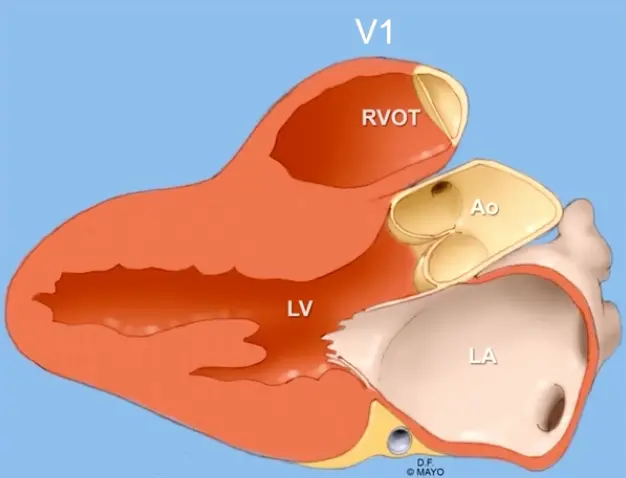
Lead V1
V1 is located on the anterior part of the chest (and is a rightward lead)
can help localize the portion of the RVOT the VT is exiting from.
QS pattern is found in V1 → anterior RVOT wall origin
rS pattern is seen in V1 → posterior wall of the RVOT
V1 is located anterior to the RVOT as we are accustomed to seeing on PLAX view on Echo
Records how the depolarization is going in this direction, anterior to posterior.
If the terminal part in V1 is predominantly negative, then we call it as left bundle morphology.
As the left bundle is blocked, LV activation is delayed and the activation is going from anterior to posterior (i.e. away from lead V1, ∴ negative deflection).
If the terminal part of V1 is positive, we call it as right bundle branch morphology.